

Virtual remote appointments are available. Contact us for a video telehealth evaluation.

All appointments conducted by our Board Certified doctor and not assistants or non-physician providers.
Why Fallopian Tube Recanalization before In Vetro Fertilization?
Fallopian tube recanalization is the least invasive and most affordable option in restoring fertility in a hopeful mother with blocked fallopian tubes. In Vitro Fertilization (IVF) can cost 20-30 times the cost of fallopian tube recanalization with similar success rate for pregnancy (see below). This minimally invasive outpatient procedure (described below) should be attempted first before pursuing IVF. If successful a patient has a chance at a natural pregnancy. However, if the blocked fallopian tube cannot be opened a patient then knows that their only option is IVF. This outpatient procedure can not only help hopeful mothers understand what their path to pregnancy is but can potentially save 10s of thousands of dollars in the process.
Fallopian Tube Blockage
Fallopian tube blockage is one of the most common causes of female infertility. The fallopian tubes are very fine tube-like structures that connect the ovaries on either side to the uterus. The eggs from the ovaries normally travel through the fallopian tubes, where they can be met and fertilized by sperm. Sometimes the tubes can become blocked or narrowed, preventing pregnancy. This can happen in one or both fallopian tubes.
Fallopian tube recanalization is a minimally invasive treatment for blocked or narrowed fallopian tubes and much more affordable than IVF. The procedure is possible in 90% of women with proximal tube occlusion (blockage of the fallopian tube near the uterus).1 The American Society for Reproductive Medicine recommends recanalization before attempting more invasive and more expensive fertility treatments like IVF.1 The tubes are recanalized through a procedure called fallopian tube catheterization with selective salpingography.
Fallopian tube recanalization is indicated in patients who are unwilling to undertake the emotional stress and expense of IVF, those who do not wish to receive hormonal stimulation, or those who are not good candidates for IVF (for example, due to advanced maternal age).5 In such patients, fallopian tube recanalization is a good option as a first-line treatment to help them get pregnant.
How is Fallopian Tube Recanalization Performed?
We can diagnose and treat blocked fallopian tubes with selective salpingography, which is a non-surgical procedure. It is usually done between days 7 and 12 of the menstrual cycle. You will need to stop eating and drinking 8 hours prior. You will be given moderate sedation through an IV to make you comfortable for the procedure and alleviate any anxiety. We start antibiotic prophylaxis (preventive treatment) 2 days before the procedure.
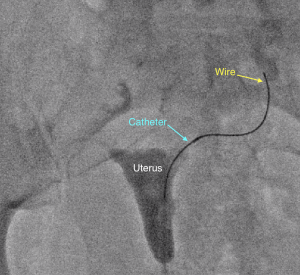
During the procedure, similar to a pelvic exam at your OBGYN, you lay on your back and a speculum is placed into the vagina. Then a small catheter is inserted through the cervix and a contrast agent, or dye, is injected into the uterus so an X-ray image of the uterine cavity can be obtained. When a fallopian tube blockage is identified, another smaller catheter and wire are threaded into the fallopian tube to open the blockage.
Our outpatient center sees patients that travel from not only the Los Angeles area but throughout the West Coast seeking our specialists' expertise. The procedure is performed by our Interventional Radiologist who is board certified in image-guided procedures using X-rays, tiny catheters and other micro-tools. What is Interventional Radiology? This is the only specialty in medicine specifically trained to perform image-guided minimally invasive procedure. Read more here.
What Causes Tubal Blockage?
As noted, the fallopian tubes are fine, tube-like structures. They are about 7-9 cm long and 1 mm in diameter.1 Because of their fine size, the fallopian tubes are prone to becoming blocked due to accumulation of debris or scarring following inflammation.
The most common cause of tubal factor infertility is pelvic inflammatory disease (PID). PID is a general term used to describe inflammation of the uterus, fallopian tubes, and sometimes the ovaries. It is generally caused by repeated sexually transmitted infections (STIs) such as chlamydia or gonorrhea (although this is not always the case). If left untreated, scar tissue can build up, leading to the blockage of one or both fallopian tubes, causing infertility. If only one tube is blocked, you may still be able to conceive naturally depending on the health of the ovary on that side.
Other causes of tubal factor infertility include:
• Endometriosis
• Previous ectopic pregnancy
• Previous abdominal surgery
• History of infection caused by miscarriage or abortion
• Previous or current infection with gonorrhea or chlamydia
Although tuberculosis is relatively rare in the Western world, it can also cause infection in the fallopian tubes, as can a ruptured appendix. All of these can cause scar tissue, mucus and debris to build up in the fallopian tubes, which can lead to blockage.
What Factors Affect Fertility After Fallopian Tube Recanalization?
Various factors can affect pregnancy rates following fallopian tube recanalization:
• Age: Chances of conception are higher in women under the age of 35.2,4
• Type of infertility: Women with secondary infertility are 15 times more likely to conceive compared to women with primary infertility.2 Primary infertility refers to couples who have not got pregnant after at least one year of unprotected sex. Secondary infertility refers to couples who were previously able to get pregnant but now are unable.
• Duration of infertility: Recanalization is 21 times more likely to succeed if infertility is less than 5 years’ duration compared to infertility of longer duration.
• Number of recanalized tubes: The chances of success are higher when both tubes are blocked and recanalized compared to when the tube on only one side is blocked and recanalized. In patients with one blocked tube and one good tube, other factors may be contributing to infertility.
• History of prior interventions: Women with a prior placement of intrauterine device, uterine dilatation and curettage (D&C), induced abortion and other such interventions have a higher pregnancy rate following fallopian tube recanalization.
• Prior successful conception: Women who have had prior successful conception have a higher chance of becoming pregnant after treatment with fallopian tube recanalization compared to women who have never been pregnant.
The success rate of fallopian tube recanalization also depends on the anatomy of the fallopian tube. The portion of the tube closest to the uterus is tiny (approximately 1 mm in diameter) and can be straight, slightly curved, or tortuous (with multiple twists and turns). This unique anatomy puts the fallopian tube at risk of accumulating debris or becoming scarred from inflammation, leading to obstruction and infertility.
What is the Success Rate?
The pregnancy rate after fallopian tube recanalization is high. Studies show that 6 out of 10 patients can conceive if the unblocked tubes are normal, i.e., there is no underlying tubal disease.
If the blockage is due to debris within the tube, there is a high chance of success. Debris within the tube usually causes blockage of the proximal fallopian tube (near the uterus).
If the tube is scarred down from prior infection or inflammation, there is a lower success rate of opening the blockage. Pelvic inflammatory disease (PID) often causes distal fallopian tube blockage (near the ovary). It’s much simpler to fix a clogged pipe than a broken pipe.
The technical success rate of fallopian tube catheterization is extremely high (up to 100%). 2 However, sometimes, tubal re-occlusion occurs, i.e., the fallopian tubes become blocked again. This occurs in 50% of patients who do not conceive by 6 months. Such patients may benefit from a repeat catheter recanalization. Pregnancy can occur after a second or even a third fallopian tube recanalization. It is also worth noting that once the tubes are open, additional fertility treatments may be necessary.
Selective salpingography and fallopian tube recanalization is a safe and effective treatment. Success rates are high in experienced hands with dedicated equipment in the appropriate setting.
Fallopian Tube Recanalization Cost
We do not accept insurance for the FTR procedure. Please contact our office for the current charges.
Why Choose Our Specialist for Fallopian Tube Recanalization?
Superior catheter and wire skills is essential in a delicate procedure such as fallopian tube recanalization. Our doctor is an image-guided specialist having performed over 5,000 procedures with experience in not only fallopian tube recanalization but also in recanalization of blocked veins and arteries. This wide array of experience brings a unique set of skills to ensure that you have the most successful outcome.
We have a high success rate at CVI not only because our physician is expertly skilled but also because we provide the physician with the best tools needed to open the fallopian tubes. The choice of wires and catheters that are placed through the fallopian tubes are essential to provide you the best chance at success. Unlike other clinics you can rest assured that at CVI we do not cut corners and only purchase the best and highest quality tools that our specialist requires.
Appointments are available via an online video telehealth platform or in person at one of the offices in Los Angeles, Orange County or San Diego, depending on the doctor’s availability. Contact Us Today. Why should you choose us? Read here.
References:
1. Thurmond AS. Fallopian tube catheterization. Semin Intervent Radiol. 2008;25(4):425-431. doi:10.1055/s-0028-1102995 Available online. Accessed on August 30, 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3036530/
2. Al-Omari MH, Obeidat N, Elheis M, Khasawneh RA, Gharaibeh MM. Factors Affecting Pregnancy Rate Following Fallopian Tube Recanalization in Women with Proximal Fallopian Tube Obstruction. J Clin Med. 2018;7(5):110. Published 2018 May 10. doi:10.3390/jcm7050110 Available online. Accessed on August 30, 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5977149/
3. Al-Omari M, Al-Mnayyis A, Obeidat N, et al. Fallopian tube recanalisation using dedicated radiographic tubal assessment set in angiography suite. J Med Imaging Radiat Oncol. 2014;58(4):415-421. doi:10.1111/1754-9485.12169 Available online. Accessed on August 30, 2020. https://pubmed.ncbi.nlm.nih.gov/24592879/
4. Papaioannou S, Afnan M, Girling AJ, et al. Long-term fertility prognosis following selective salpingography and tubal catheterization in women with proximal tubal blockage. Hum Reprod. 2002;17(9):2325-2330. doi:10.1093/humrep/17.9.2325 Available online. Accessed on August 30, 2020. https://pubmed.ncbi.nlm.nih.gov/12202420/
5. Knuttinen MG, Jajko R, Scoccia B. Fluoroscopic tubal recanalization in tubal factor related infertility. Semin Intervent Radiol. 2014;31(3):269-271. doi:10.1055/s-0034-1382797 Available online. Accessed on August 30, 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4139428/
The above information explains what is involved and the possible risks. It is not meant to be a substitute for informed discussion between you and your doctor, but can act as a starting point for such a discussion.